
All product descriptions and articles provided on this website are intended strictly for informational and educational purposes. Our products are designed exclusively for in-vitro research (i.e., experiments conducted outside of a living organism, typically in glassware such as test tubes or petri dishes). These compounds are not approved by the FDA for use in humans or animals. They are not medications, nor are they intended to diagnose, treat, prevent, or cure any disease or medical condition. Any bodily administration-human or animal-is strictly prohibited by law. Our products are not for human consumption under any circumstances.
TB-500 for Pulmonary Fibrosis: Shifting the Repair Paradigm
Current antifibrotic drugs slow scarring but fail to restore damaged lungs, leaving a critical gap in pulmonary fibrosis care.TB-500 matters because it targets mechanisms beyond fibrosis suppression. Preclinical data suggest it promotes epithelial healing, regulates fibroblast activity, and enhances angiogenesis. Unlike current drugs that merely slow decline, TB-500 could actively restore lung structure and function if validated in clinical trials.
However, despite promising animal data, translation to clinical settings remains uncertain. Optimal dosing, long-term safety, and delivery methods must be validated through well-designed human trials. Without these studies, TB-500’s true potential in fibrosis therapy cannot be fully determined.
Why are peptides getting attention for fibrotic lung disease?
Peptides are gaining attention in fibrotic lung disease because they directly target repair pathways neglected by conventional drugs. Their ability to regulate fibroblasts, modulate inflammation, and stimulate angiogenesis makes them promising candidates for reversing scarring, not just slowing disease progression.
Additionally, peptides like TB-500 offer higher specificity, lower toxicity, and potential synergy with existing antifibrotics. By mimicking natural biological signals, they may restore tissue balance more effectively, positioning peptide-based therapeutics as a frontier in pulmonary fibrosis research.
What is TB-500, and why does it matter now?
TB-500 is a synthetic peptide fragment of thymosin β-4, designed to promote tissue regeneration and regulate inflammation. It matters now because existing antifibrotics fail to reverse scarring, while TB-500 shows potential to repair damaged lung tissue at a cellular level.
Growing preclinical evidence highlights TB-500’s ability to reduce collagen buildup, enhance angiogenesis, and restore alveolar structure in fibrosis models. With pulmonary fibrosis cases rising worldwide, its regenerative promise positions TB-500 as an urgent research priority for novel therapies.
Preclinical signals worth noting
Preclinical evidence shows TB-500 reduces collagen deposition, regulates fibroblasts, lowers inflammation, and enhances angiogenesis across cardiac, muscle, and lung fibrosis models, signalling strong regenerative potential but requiring human clinical validation.
Lung models: protective, immunomodulatory effects. Multiple bleomycin and LPS injury studies [1] show that Tβ4 or related fragments reduce lung inflammation, lower collagen accumulation, and preserve alveolar structure in mice. These experiments demonstrate reduced leukocyte infiltration, less hydroxyproline (collagen) content, and improved histology after Tβ4 treatment.
Local delivery shows promise: Aerosolized or nebulized recombinant Tβ4 administered directly to the lung improved outcomes in murine bleomycin models [2] and inhibited fibroblast activation in vitro, supporting inhalation as a pragmatic delivery route for lung disease.
Fragment biology (Ac-SDKP and related peptides). Short fragments derived from larger thymosin sequences, notably Ac-SDKP, display potent anti-fibrotic activity in fibroblast cultures and in vivo models, sometimes outperforming full-length Tβ4 in suppressing TGF-β-driven activation. These results [3] point toward fragment optimization as a useful strategy.
Cross-organ regenerative evidence. Cardiac and muscle injury studies [4] repeatedly show that Tβ4-based peptides reduce scar size, improve vascularization, and accelerate functional recovery, mechanistic findings that provide biological plausibility for lung translation.
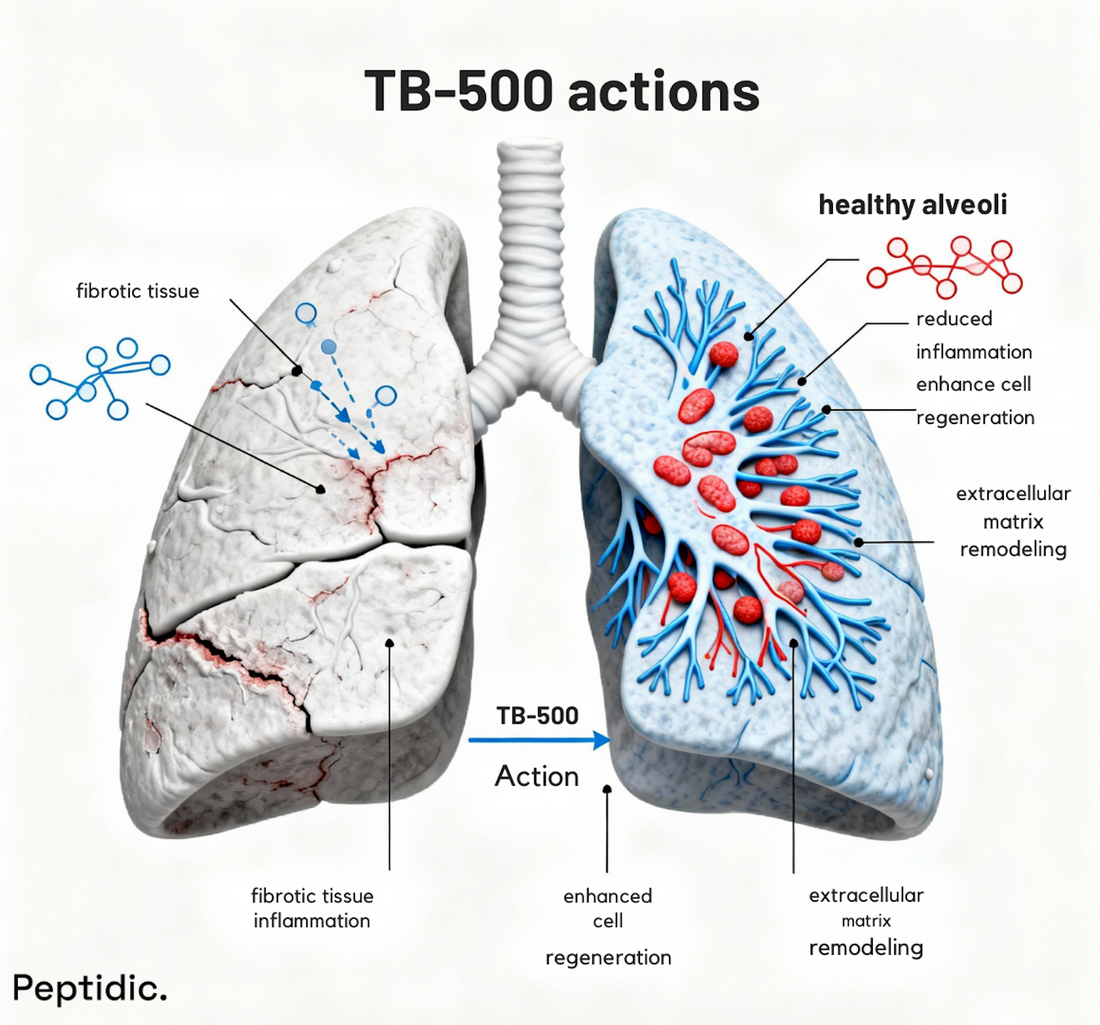
How TB-500 appears to work
TB-500 appears to work by regulating actin polymerization, enhancing epithelial repair, modulating fibroblast activity, and promoting angiogenesis, collectively reducing scarring and supporting regenerative healing in fibrotic lung disease models.
- Actin modulation & cell migration: TB-500 enhances epithelial and endothelial cell movement to repopulate damaged areas.
- Fibroblast regulation: It dampens myofibroblast activation and markers such as α-SMA in several models.
- Immune rebalancing: Studies report reductions in pro-fibrotic cytokines (e.g., IL-17) and shifts in inflammatory cell populations that favour resolution over chronic activation.
- TGF-β pathway interaction: Evidence suggests TB-500 and fragments can interfere with TGF-β [3] signalling cascades that drive fibrosis.

Formulation & delivery strategies researchers should prioritize.
Researchers should prioritize inhaled delivery, AAV-mediated expression, and short-fragment analogues for targeted lung therapy. Nanoparticles, exosomes, and controlled-release systems can further enhance stability, bioavailability, and sustained anti-fibrotic effects.
1- Nebulized/inhaled protein or peptide: Direct lung delivery concentrates the effect, reduces systemic exposure, and shows efficacy in mice.
2- AAV or gene-delivery vectors for localized expression: AAV-mediated Tβ4 expression reduced LPS-driven lung injury in murine studies [5], suggesting vectorized approaches for chronic disease models.
3- Short-fragment optimization (Ac-SDKP analogues): Smaller sequences may offer better tissue penetration and more predictable anti-fibrotic activity.
Key translational hurdles (what stops us from moving to patients).
Major translational hurdles include the absence of large-scale human trials, unclear optimal dosing, limited delivery strategies, and insufficient long-term safety data, all preventing TB-500 from advancing reliably into pulmonary fibrosis patient care.
- Human safety and dosing: Most evidence is preclinical; human PK/PD and chronic-use safety are unknown. Only a few small clinical studies [6] on thymosin peptides exist outside fibrosis, so careful phase-I work is essential.
- Heterogeneity of fibrosis: IPF, post-TB fibrosis, and drug-induced scarring differ biologically; one peptide dose/regimen might not fit all.
- Biomarkers & endpoints: Trials need sensitive, repair-oriented endpoints (imaging biomarkers, functional alveolar measures, molecular markers of epithelial regeneration) rather than just FVC decline.
- Manufacturing & stability: Peptide aggregation, aerosol stability, and scalable GMP production must be addressed early.
Why partner with Peptidic (if you’re a researcher)?
Partnering with Peptidic gives researchers access to premium-grade TB-500 peptides backed by rigorous quality control and scientific expertise. Our compounds are designed to deliver reliable, reproducible results, enabling scientists to accelerate fibrosis research with confidence and precision.
Beyond supplying peptides, Peptidic provides tailored research support, helping investigators design and refine fibrosis models. By combining innovation with reliability, we empower researchers to explore regenerative therapies like TB-500 and push the boundaries of pulmonary fibrosis treatment discovery.
Advance Your Fibrosis Research with Peptidic
Pulmonary fibrosis researchers face a constant struggle: limited tools, therapies that only slow progression, and peptides of inconsistent quality that compromise reproducibility. These challenges delay discoveries and make it harder to translate promising mechanisms like TB-500 into meaningful clinical outcomes.
At Peptidic, we solve this problem by providing premium-grade TB-500 and other advanced peptides manufactured under rigorous standards. Backed by scientific expertise and tailored research support, we help you generate reliable results, accelerate fibrosis breakthroughs, and move closer to real-world therapies.

FAQs:
Can TB-500 be combined with other pulmonary fibrosis therapies?
TB-500 may complement antifibrotic drugs like pirfenidone and nintedanib by promoting repair and reducing inflammation. While this combination looks promising mechanistically, it remains theoretical until safety, synergy, and clinical benefit are validated through controlled human trials.
What biological pathways does TB-500 influence in fibrosis?
TB-500 regulates actin polymerization, aiding cell migration, angiogenesis, and tissue repair. It also modulates fibroblast activity, epithelial regeneration, and TGF-β signalling. By targeting both inflammation and fibrosis, it offers a broader therapeutic scope than conventional antifibrotic drugs.
Is TB-500 safe for long-term use in humans?
No long-term human safety data exist for TB-500. Animal studies show favourable effects with low toxicity, but human physiology differs. Controlled phase trials assessing dosage, chronic exposure, and organ safety are essential before therapeutic adoption.
Could TB-500 benefit post-tuberculosis lung damage?
TB-500 could address post-TB fibrosis by reducing collagen deposition, controlling residual inflammation, and enhancing alveolar repair. Early preclinical data support this potential, but targeted clinical studies are necessary to confirm efficacy and safety in post-tuberculosis patients.
References

